REPRODUCTIVE HEALTH
- World Health Organisation (WHO) Define REPRODUCTIVE HEALTH as “a total well-being in all aspects of reproduction, i.e., physical, emotional, behavioural and social”
- UN agencies claim sexual and reproductive health includes physical, as well as psychological well-being vis-a-vis sexuality.
- Reproductive health implies that people are able to have a responsible, satisfying and safer sex life and that they have the capability to reproduce and the freedom to decide if, when and how often to do so. One interpretation of this implies that men and women ought to be informed of and to have access to safe, effective, affordable and acceptable methods of birth control; also access to appropriate health care services of sexual, reproductive medicine and implementation of health education programs to stress the importance of women to go safely through pregnancy and childbirth could provide couples with the best chance of having a healthy infant.
- According to the United Nations Population Fund (UNFPA), unmet needs for sexual and reproductive health deprive women of the right to make “crucial choices about their own bodies and futures”, affecting family welfare. Women bear and usually nurture children, so their reproductive health is inseparable from gender equality. Denial of such rights also worsens poverty.
- Components of reproductive health
- Knowledge about reproductive organs,Adolescent health,Maternal health,Contraception,Sexually transmitted infection,Abortion,Female genital .
- Child and forced marriage.
- REPRODUCTIVELY HEALTHY SOCIETY
- A society with people having physically and functionally normal reproductive organs and normal emotional and behavioural interactions among them in all sex-related aspects
FAMILY PLANNING PROGRAMMES
- India was amongst the first countries in the world to initiate action plans and programmes at a national level to attain total reproductive health as a social goal.
- These programmes called ‘family planning’ Initiated in 1951
- Improved programmes covering wider reproduction-related areas à Reproductive and Child Health Care (RCH) programmes.
- Reproductive Child Health (RCH)
- Improving maternal and child health has been one of the top health priorities of Government of India.In view of this, The Reproductive and Child Health (RCH) 1 Programme was launched throughout the country on 15th October, 1997.The second phase of RCH program i.e. RCH – II was launched on 1st April, 2005.
- The main objective of the program was to bring about a change in mainly three critical health indicators i.e. reducing total fertility rate, infant
- mortality rate and maternal mortality rate with a view to realizing the outcomes envisioned in the Millennium Development Goals.
- RMCH+A approach has been launches in 2013 and it essentially looks to address the major causes of mortality among women and children as well as the delays in accessing and utilizing health care and services.
- To add to this various programs and schemes has been launched by Government of India to achieve reproductive health goals.
AIM FOR FAMILY PLANNING PROGRAMMES
- CREATING AWARENESS among people about various reproduction related aspects
- Proper information about reproductive organs, adolescence and related changes, safe and hygienic sexual practices, sexually transmitted diseases ,Educating people, especially fertile couples and those in marriageable
- age group, about available birth control options,
- Care of pregnant mothers, post-natal care of the mother and child
- Importance of breast feeding,
- Equal opportunities for the male and the female child, etc.,
- PROVIDING FACILITIES AND SUPPORT for building up a reproductively healthy society
- HOW GOVERNMENT CREATED AWARENESS?
- With the help of audio-visual & the print-media
- NGOs Involvement to reach masses
- Parents, other close relatives, teachers and friends, also have a major role in the dissemination of the above information.
- Introduction of sex education in schools
HOW REPRODUCTIVE HEALTH INFORMATION IS HELPFUL?
- It would help people, especially those in the adolescent age group to lead a reproductively healthy life.
- It would address the importance of bringing up socially conscious healthy families of desired size.
- Awareness of problems due to uncontrolled population growth, social evils like sex-abuse and sex-related crimes, etc., need to be created to enable people to think and take up necessary steps to prevent them and thereby build up a socially responsible and healthy society.
HOW TO IMPLEMENT REPRODUCTIVE HEALTH RELATED PROGRAMME SUCCESSFULLY?
- Better ground level facilities (Better infrastructure) required
- Professional expertise (doctors, trained nurses & trained staff) required
- Material support (Easily understandable, regional language, more convincing promotional material & training kit)
- Medical assistance and care to people
- in reproduction-related problems like pregnancy, delivery, STDs, abortions, contraception, menstrual problems, infertility, etc.
- Implementation of better techniques and new strategies
- to provide more efficient care and assistance to people.
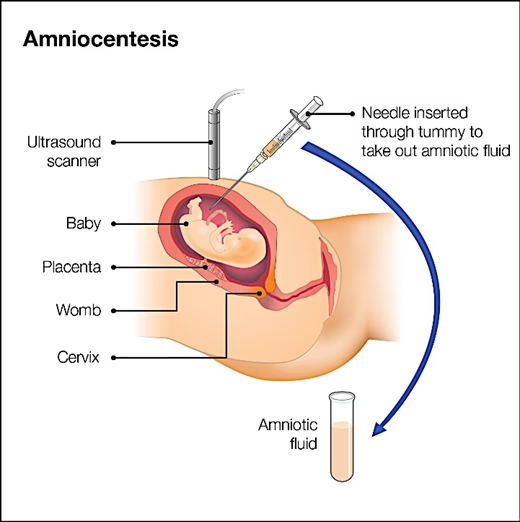
- STATUTORY BAN ON AMNIOCENTESIS
- A foetal sex determination test based on the chromosomal pattern in the amniotic fluid surrounding the developing embryo
- Misused for sex-determination leads to increasing female foeticides
- Massive child immunisation to prevent child mortality
- Research on various reproduction-related areas are encouraged (New one or improve existing one)
- The main indications for amniocentesis include:
- Karyotyping
- haemolytic disease
- maturity of foetal lungs
- biochemical studies
WHAT IS ‘SAHELI’?
- A new oral contraceptive for the females
- Developed by Central Drug Research Institute (CDRI) in Luc know, India
- Saheli is Non Hormonal contraceptive
- Once a week pill
- Active chemical Centchroman (Ormeloxifen).
- It is a Selective Estrogen Receptor Modulator, (SERM) a class of medication which act on estrogen receptors.

- POSITIVE OUTCOMES OF REPRODUCTIVE HEALTH PROGRAMMES:
- Better awareness about sex related matters,
- Decreased maternal and infant mortality rates
- Increased number of medically assisted deliveries and
- Better post-natal care
- Increased number of couples with small families,
- Better detection and cure of STDs
- Overall increased medical facilities for all sex-related problems, etc.
- Improved reproductive health of the society.
- POSITIVE OUTCOMES OF REPRODUCTIVE HEALTH PROGRAMMES:
- Better awareness about sex related matters,
- Decreased maternal and infant mortality rates
- Increased number of medically assisted deliveries and
- Better post-natal care
- Increased number of couples with small families,
- Better detection and cure of STDs
- Overall increased medical facilities for all sex-related problems, etc.
- Improved reproductive health of the society.
- CONTRACEPTIVE METHODS
- Purpose à Help to prevent unwanted pregnancies.
- AN IDEAL CONTRACEPTIVE SHOULD BE
- user-friendly,
- easily available,
- effective and
- reversible with no or least side-effects.
- not interfere with the sexual drive, desire and/or the sexual act
- Range of contraceptive methods are presently available
- Natural/Traditional, Barrier,
- IUDs,
- Oral contraceptives,
- Injectables,
- Implants and
- Surgical methods.
- NATURAL METHODS OF CONTRACEPTION:
- Principle of avoiding chances of ovum and sperms meeting.
- PERIODIC ABSTINENCE
- The couples avoid or abstain from coitus (sex) from DAY 10 TO 17 of the menstrual cycle (fertile period)
- WITHDRAWAL OR COITUS INTERRUPTUS
- The male partner withdraws his penis from the vagina just before ejaculation so as to avoid insemination.
- LACTATIONAL AMENORRHEA METHOD
- Based on the fact that ovulation do not occur during the period of intense lactation
- Effective only up to a maximum period of SIX MONTHS following parturition.
- Advantages As no medicines or devices are used in these methods, side effects are almost nil.
- Disadvantages is Chances of failure high.
- BARRIER METHODS OF CONTRACEPTION:
- Ovum and sperms are prevented from physically meeting with the help of barriers.
- Such methods are available for both males and females.
- Protecting the user from contracting STDs and AIDS.
- Both the male and the female condoms are disposable, can be self- inserted and thereby gives privacy to the user.
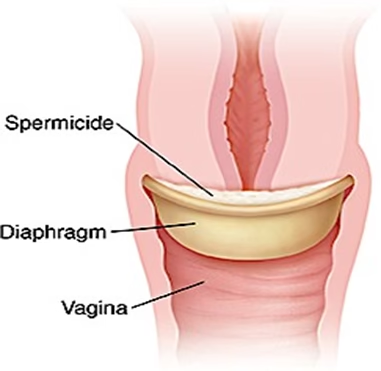
- DIAPHRAGMS, CERVICAL CAPS AND VAULTS
- Barriers made of rubber
- Inserted into the female reproductive tract to cover the cervix during coitus.
- They prevent conception by blocking the entry of sperms through the cervix.
- They are reusable.
- Spermicidal creams, jellies and foams are usually used along with these barriers to increase their contraceptive efficiency.
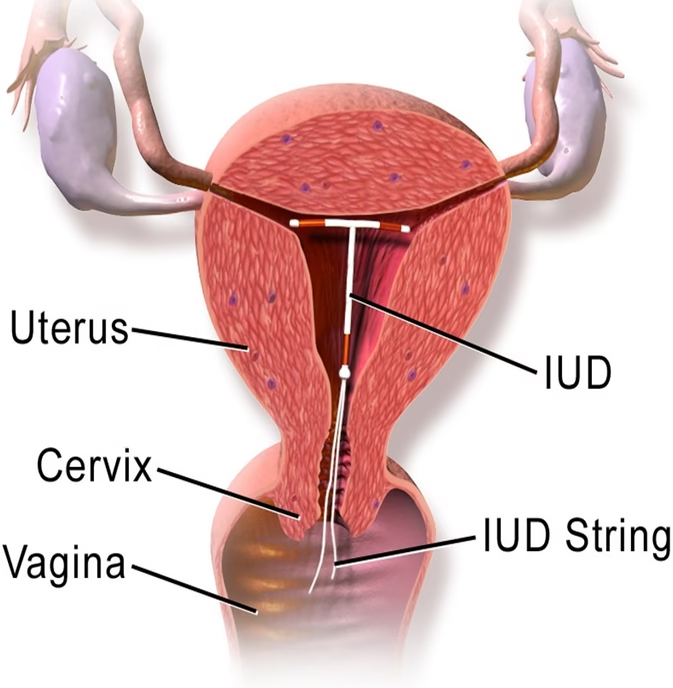
- INTRA UTERINE DEVICES (IUDS).
- These devices are inserted by doctors or expert nurses in the uterus through vagina.
- These Intra Uterine Devices are presently available as
- The non-medicated IUDs -Lippes loop,Copper releasing IUDs -CuT, Cu7, Multiload 375
- Hormone releasing IUDs – Progestasert, LNG-20
- MECHANISM OF IUD
- IUDs increase PHAGOCYTOSIS OF SPERMS within the uterusCu ions released SUPPRESS SPERM MOTILITY and the fertilising capacity of sperms.
- The hormone releasing IUDs MAKE THE UTERUS UNSUITABLE FOR IMPLANTATION and the cervix hostile to the sperms.
- IUDs are ideal contraceptives for the females who want to delay pregnancy and/or space children.
- Generally THIS METHOD not used for unmarried girls or newly married (having no kids)
- It is one of most widely accepted methods of contraception in India.
- PILLS / ORAL CONTRACEPTIVES:
- Oral administration
- Small doses of either progestogens or progestogen–estrogen combinations
- Contraceptive method used by the females.
- Pills have to be taken daily for a period of 21 days starting preferably within the first five days of menstrual cycle.
- After a gap of 7 days (during which menstruation occurs) it has to be repeated in the same pattern till the female desires to prevent conception.
- How it works?
- They inhibit ovulation and implantation
- Alter the quality of cervical mucus to prevent/ retard entry of sperms.
- Pills are very effective with lesser side effects and are well accepted by the females.After a gap of 7 days (during which menstruation occurs) it has to be repeated in the same pattern till the female desires to prevent conception.
- How it works?
- They inhibit ovulation and implantation
- Alter the quality of cervical mucus to prevent/ retard entry of sperms.
- Pills are very effective with lesser side effects and are well accepted by the females.
- IMPLANTS / INJECTIONS:
- Progestogens alone or in combination with oestrogen can also be used by females as injections or implants under the skin
- Their mode of action is similar to that of pills and their effective periods are much longer.
- EMERGENCY CONTRACEPTION à
- Administration of progestogens or progestogen – oestrogen combinations or IUDs “WITHIN 72 HOURS OF COITUS”
- Very effective as emergency contraceptives
- Could be used to avoid possible pregnancy due to rape or casual unprotected intercourse.
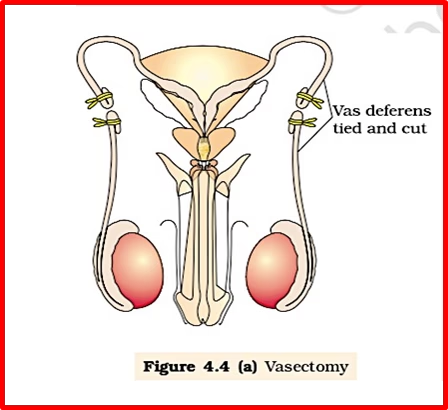
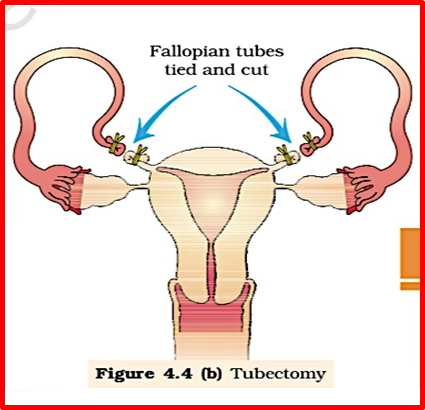
- SURGICAL METHODS (STERILISATION)
- Terminal method to prevent any more pregnancies.
- Surgical intervention blocks gamete transport and thereby prevent conception.
- Sterilisation procedure
- in the male is called ‘VASECTOMY’
- in the female, ‘TUBECTOMY’.
- VASECTOMY, a small part of the vas deferens is removed or tied up through a small incision on the scrotum
- In TUBECTOMY, a small part of the fallopian tube is removed or tied up through a small incision in the abdomen or through vagina.
- These techniques are highly effective but their reversibility is very poor.
- CONTRACEPTION ADVICE:
- The selection of a suitable contraceptive method and its use should always be undertaken in consultation with qualified medical professionals.
- One must also remember that contraceptives are not regular requirements for the maintenance of reproductive health.
In fact, they are practiced against a natural reproductive event, i.e., conception/pregnancy
- MEDICAL TERMINATION OF PREGNANCY (MTP)
- Intentional or voluntary termination of pregnancy before full term
- Also called induced abortion.
- Nearly 45 to 50 million MTPs / a year all over the world ( 1/5th of the total number of conceived pregnancies in a year)
- MTP has a significant role in decreasing the population though it is not meant for that purpose.
- Government of India legalised MTP in 1971 with some strict conditions to avoid its misuse.
- Such restrictions à to check female foeticides
- THE MEDICAL TERMIN ATION OF PREGNANCY (AMENDMENT) ACT, 2017
- Enacted by the government of India with the intension of reducing the incidence of illegal abortion and consequent maternal mortality and morbidity.
- According to this Act, a pregnancy may be terminated on certain considered grounds within the first 12 weeks of pregnancy on the opinion of one registered medical practitioner.
- If the pregnancy has lasted more than 12 weeks, but fewer than 24 weeks, two registered medical practitioners must be of the opinion, formed in good faith, that the required ground exist.
- The grounds for such termination of pregnancies are:
- The continuation of the pregnancy would involve a risk to the life of the pregnant woman or of grave injury physical or mental health; or
- There is a substantial risk that of the child were born, it would suffer from such physical or mental abnormalities as to be seriously handicapped
- Why MTP ?
- to get rid of unwanted pregnancies either due to casual unprotected intercourse or failure of the contraceptive used during coitus or rapes.
- MTPs are also essential in certain cases where continuation of the pregnancy could be harmful or even fatal either to the mother or to the foetus or both.
- MTPs are considered relatively safe during the first trimester, i.e., upto 12 weeks of pregnancy.
- Second trimester abortions are much more riskier.
- PROBLEM with MTP –
- a majority of the MTPs are performed illegally by unqualified quacks (unsafe but could be fatal)
- Misuse of amniocentesis to determine the sex of the unborn child. à if the foetus is found to be female, it is followed by MTP (Illegal act; Punishable offence)
- SEXUALLY TRANSMITTED DISEASES (STDs)
- Infections transmitted through sexual intercourse
- Also called venereal diseases (VD) or reproductive tract infections (RTI).
- Common STDs
- Gonorrhoea,Syphilis,Genital herpes,Chlamydiasis,Genital warts,Trichomoniasis,Hepatitis-B and
- HIV leading to AIDS
- Among these, HIV infection is most dangerous
- Except for hepatitis-B, genital herpes and HIV infections, other diseases are completely curable if detected early and treated properly.
- Early symptoms of most of STD
- Itching,Fluid discharge,
- Slight pain, swellings, etc., in the genital region.
- Infected females may often be asymptomatic and hence, may remain undetected for long.
- Absence or less significant symptoms in the early stages of infection and the social stigma attached to the STDs, deter the infected persons from going for timely detection and proper treatment.
- Complications of STDs
- Pelvic inflammatory diseases (PID),Abortions,Still births,Ectopic pregnancies,Infertility or
- Cancer of the reproductive tract.
- STDs are a major threat to a healthy society. à prevention or early detection and cure of these diseases are given prime consideration
- STDs high incidences In persons of the age group of 15-24 (Adolescent & Young adults)
- One could be free of these infections by following the simple principles –
- Avoid sex with unknown partners/multiple partners.Always use condoms during coitus.
- Take advice of doctor for early detection and Treatment
- INFERTILITY
- Couples are infertile, i.e., they are unable to produce children in spite of unprotected sexual co- habitation.
- The reasons for this à physical, congenital, diseases, drugs, immunological or even psychological.
- Male or Female – anyone can have problem (Not only female)
- Specialised health care units (infertility clinics, etc.)
- For diagnosis
- For corrective treatment of infertility
- To enable couples to have children.
- If corrections are not possible then
- Special techniques are used for couples à Assisted reproductive technologies (ART)
- ASSISTED REPRODUCTIVE TECHNOLOGIES
Called IUT – intra uterine transfer
- GIFT (GAMETE INTRA FALLOPIAN TRANSFER)
- Transfer of an ovum collected from a donor into the fallopian tube (GIFT – GAMETE INTRA FALLOPIAN TRANSFER) of another female who cannot produce one, but can provide suitable environment for fertilisation and further development
- ICSI à INTRA CYTOPLASMIC SPERM INJECTION (ICSI) is specialised procedure to form an
embryo in the laboratory in which a sperm is directly injected into the ovum.
- AI ARTIFICIAL INSEMINATION (AI) treat infertility cases either due to inability of the male partner to inseminate the female or due to very low sperm counts in the ejaculates. The semen collected either from the husband or a healthy donor is artificially introduced either into the vagina or into the uterus (IUI – intra-uterine insemination) of the female.

